|
|
|
|
|
|
 Hello, and happy fall! Many people have had to make significant changes in their lives over the last six months due to the pandemic’s ever-changing status. It is apparent, now more than ever, that health is not just about a medical provider and a patient sitting in an exam room. Health is about where you work, live, play, educate, and socialize. Health is also driven
by social and economic opportunities and access to resources such as food, water, shelter, and transportation. Community health centers (CHCs) are driven by their mission to provide affordable, accessible, and high-quality care to all. Long before COVID-19 hit, CHCs have been addressing barriers to care, or social determinants of health, for the patients in their communities. Health centers can meet patients where they are at, assess, and address patients’ needs through enabling services right at the appointment time. Enabling services are non-clinical services aimed at breaking down barriers to access care and improve people’s health outcomes. Some examples of these
services are:- Transportation;
- Interpretation;
- Health insurance eligibility;
- Mediation assistance; and,
- Housing security.
Due to COVID-19, our states’ population is experiencing a turbulent situation like never before. People are suddenly in a position where they aren’t feeling secure in their basic needs. CHAD and our member health centers are committed to addressing those social determinants of health by implementing an evidence-based universal screening tool, PRAPARE. Providers will screen patients during
their visit to assess any barriers to health care or healthy activities. These questions will help them gain information to help patients overcome those barriers through services within the clinic and surrounding community. It is also crucial to look at any upstream risk factors in patients’ lives, those things that could potentially put a person’s health at risk before it becomes an issue. Look to your local health center for resources in and around your community; they are there to help you! Health begins with equity.
|
|
|
|
|
|
|
|
|
CHAD CEO Shelly Ten Napel discussed the COVID-19 spike in positive cases in the Dakotas with the Public News Service.
|
|
|
|
|
Darrold Bertsch, CEO of Coal Country Community Health Center, was interviewed by Modern Healthcare regarding the temporary Families First Coronavirus Response Act (FFCRA) labor rule.
|
|
|
|
|
|
|
|
|
|
|
|
|
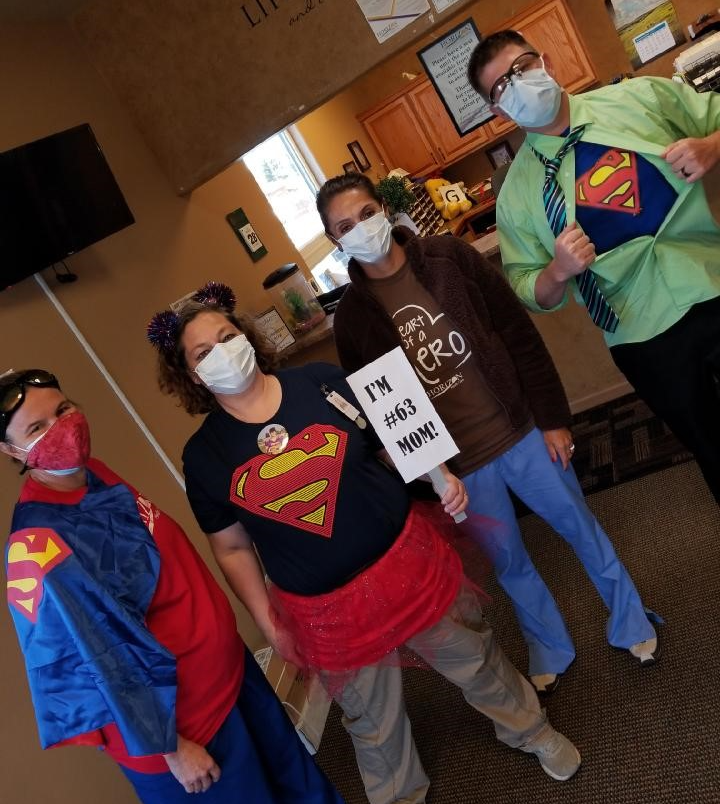
Horizon’s Martin Community Health Center staff revealed their superhero identities for the Martin Homecoming.
|
|
|
|
|
|
|
| Top Counties and Trends in the Dakotas
|
|
|
|
|
|
|
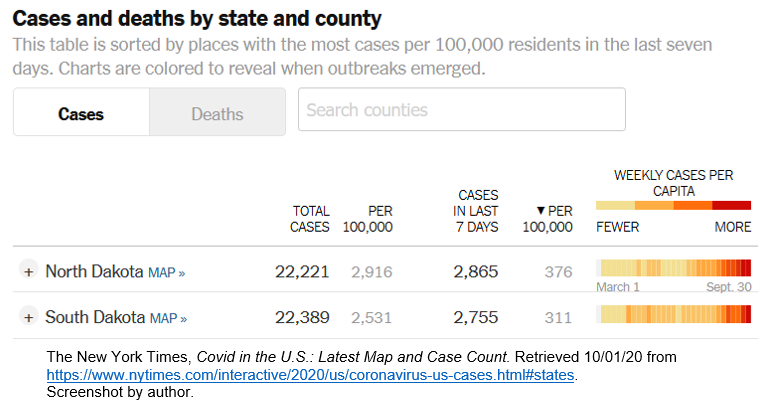
As of Wednesday, September 30, North Dakota and South Dakota are ranked numbers 1 and 2 in total new cases per population over the last seven days, according to the New York Times COVID-19 database. In North Dakota, health centers have been ramping up local testing events in
collaboration with the North Dakota Department of Health. We also see a growing impact on health center staff, with some health centers having staff unable to work due to exposures or close contacts.
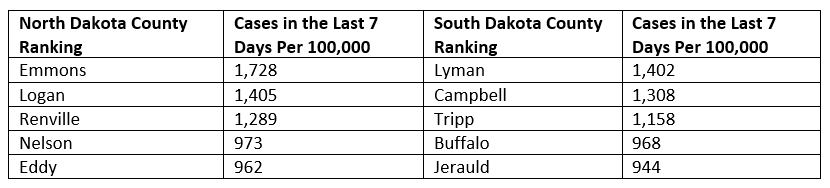
The emerging hot spots in the two states with the most cases in the last seven days per population are:
|
|
|
|
|
|
|
|
|
In South Dakota, the positivity rate over the last 14 days is 12.5%, and while recently trending
downward slightly, the positivity rate is now back on the rise. South Dakota’s cumulative positivity rate during the pandemic has also risen, to 9.1%. In North Dakota, the 14-day rolling average positivity rate is 6.96%. North Dakota’s positivity rate has been climbing since late
June when it was less than one percent. When positivity rate is considered alongside per population new cases, we can surmise that South Dakota probably currently has more cases per population than North Dakota even though South Dakota’s confirmed positives are slightly lower. South Dakota’s total positives are also likely to see a boost today (October 1) or tomorrow, because the South Dakota Department of Health has announced that, due to a computer error, they have failed to report certain positive results that have been reported to the state. Many of the recent positives reported by Horizon Health Care have been impacted in the reporting error. Here are some trusted websites that show data, trends, hospitalization rates, hot spots, etc.
|
|
|
|
|
States Differ on Hospital "Capacity" Definition and
Transparency
|
|
|
|
|
Local officials have long cited hospital capacity as the prime factor determining how North Dakota and South Dakota have been weathering the COVID-19 pandemic. But as the Dakotas have remained the top two states in the nation for positive cases
per 100,000 in September and daily positive cases and number of active cases continue to break record after record, more people have begun to scrutinize the available hospital capacity.
The Forum reported on September 29 that part of the discrepancy between the North Dakota Department of Health public-facing capacity information and what hospital representatives are reporting has to do with staffing, specifically nurses. The state has been counting licensed beds but counting staffed beds will give a more accurate picture of true capacity. Major North Dakota health systems, including Sanford, CHI St. Alexius, and Essentia, are taking measures to mitigate capacity issues, including
moving low acuity patients to smaller hospitals further away from the metro areas, increasing nursing shifts, and putting off elective procedures requiring hospital care in an effort to keep staffed beds available for COVID-19 patients. State officials met with leaders of Bismarck’s two largest hospital systems last weekend to discuss the availability of beds as the Bismarck-Mandan area, in particular,
continue to see a surge in coronavirus cases and an overall increase in COVID and non-COVID hospitalizations.
The story in South Dakota is less transparent. Representatives from the three major hospital systems, Sanford, Avera, and Monument Health, are on record saying they are not in crisis mode and have plenty of staffed beds available. While news reports and social media accounts dispute these claims, there is a lack of available information. According to Forum reports, "There is no way for South Dakotas to know how many beds the state’s three largest health systems have, where they are, how many are available, and how many are filled by patients sick with COVID-19." Available and staffed beds will remain a top concern as we move into fall and expect an increase in other respiratory conditions such as influenza in addition to COVID-19.
|
|
|
|
|
|
|
|
|
Extension of Government Funding
The President signed a Continuing Resolution (CR) late last night (September 30) to avoid a government shut-down and create a stopgap for government funding until December 11. Also included in this extension were the Community Health Center Fund, the National Health Service Corps, and the Teaching Health Centers Graduate Medical Education Program, all at current funding levels. Find a summary of the legislation here.
|
|
|
|
|
COVID-19 Stimulus Package
The House is expected to pass a $2.2 trillion COVID-19
stimulus bill this week. This vote is seen as the House’s last effort to pass a bill before the election. The House had previously passed a $3 trillion package, while the Senate failed to pass its version, a $1.2 trillion package. The National Association of Community Health Centers (NACHC) continues to press Congress to pass another bill to include the health center $7.6 billion emergency fund and telehealth language.
|
|
|
|
|
DOL Issues Revised Sick Leave Rules
On September 16, the DOL issued
revised regulations on the Families First Coronavirus Response Act’s (FFCRA) emergency paid-sick-leave (EPSLA) and the Emergency Family and Medical Leave Expansion Act (EFMLEA), which initially went into effect on March 18.
Under the EPSLA, employers with fewer than 500 employees and some public employers must pay sick leave of up to 80 hours, or roughly 10 days, to employees who need to take leave for certain coronavirus-related reasons. Employees may be eligible for an additional 10 weeks of family leave paid at two-thirds of their regular wages under the EFMLEA to care for a child whose school or place of care is closed or whose child care provider is
unavailable because of COVID-19. Health care providers were originally exempted from these requirements, although many health centers in the Dakotas elected to offer these benefits to employees.
The DOL’s revised regulations changes the definition of "health care provider" to include "only employees who meet the definition of that term under the Family and Medical Leave Act (FMLA) regulations or who are employed to provide diagnostic services, preventative services, treatment services or other services that are integrated with and necessary to the provision of patient care which, if not provided, would adversely impact patient care." The impact of this
change is that effective September 16, health centers must offer COVID-19-related leave benefits to employees not directly involved in patient care.
The revised regulations also make the following clarifications:
- Reaffirms that employees may take FFCRA leave only when work is available to them;
- Reaffirms that employees must have their employer’s approval to take intermittent FFCRA leave;
- Clarifies that employees must provide employers with documentation as soon as possible supporting their need for FFCRA leave; and,
- Corrects an inconsistency when employees may be required to provide employers notice of their need to take expanded family and medical leave.
Find the full revisions document on the Federal Register’s published documents page.
|
|
|
|
|
Executive Order on Combating Race and Sex Stereotyping
On September 22, President Trump signed an executive order (EO) which disallows certain aspects of race and gender equity training, citing that such trainings foster "divisive concepts," such as the recognition of racial and gender privilege, reparations, the belief that denying race does not discontinue racism, and the imbalance of influence in private and public sectors based on race and gender. The EO argues that such concepts are inaccurate, harmful, and misrepresent American history and doctrine.
A complete list of "divisive concepts" includes:
One race or sex is inherently superior to another race or sex;
The United States is fundamentally racist or sexist;
An individual, by virtue of his or her race or sex, is inherently racist, sexist, or oppressive, whether consciously or unconsciously;
An individual should be discriminated against or receive adverse treatment solely or partly because of his or her race or sex;
Members of one race or sex cannot and should not attempt to treat others without respect to race or sex;
An individual’s moral character is necessarily determined by his or her race or sex;
An individual, by virtue of his or her race or sex, bears responsibility for actions committed in the past by other members of the same race or sex;
Any individual should feel discomfort, guilt, anguish, or any other form of psychological distress on account of his or her race or sex; or,
Meritocracy or traits such as a hard work ethic are racist or sexist or were created by a particular race to oppress another race. The term "divisive concepts" also includes any other form of race or sex-stereotyping or sex scapegoating.
The EO directs all federal agencies to review their grant programs to determine how to condition those grants on compliance with the restriction on certain aspects of racial bias trainings. Read the full EO here with special emphasis on Sec. 5. Requirements for Federal Grants. More details are
likely to be forthcoming from the Department of Health and Human Services, but in the meantime, health centers are encouraged to be familiar with the new restrictions when considering future activities or trainings where such concepts may be shared.
|
|
|
|
|
|
|
|
|
The situation with the 340B program continues to develop daily. CHAD is working to keep members and stakeholders informed through the process. CHAD has put together a 340B distribution list for weekly updates and other training and advocacy opportunities. Email Jessica Gilbertson, policy and partnership manager, to be added to the list. A few of the updates from the last week include:
|
|
|
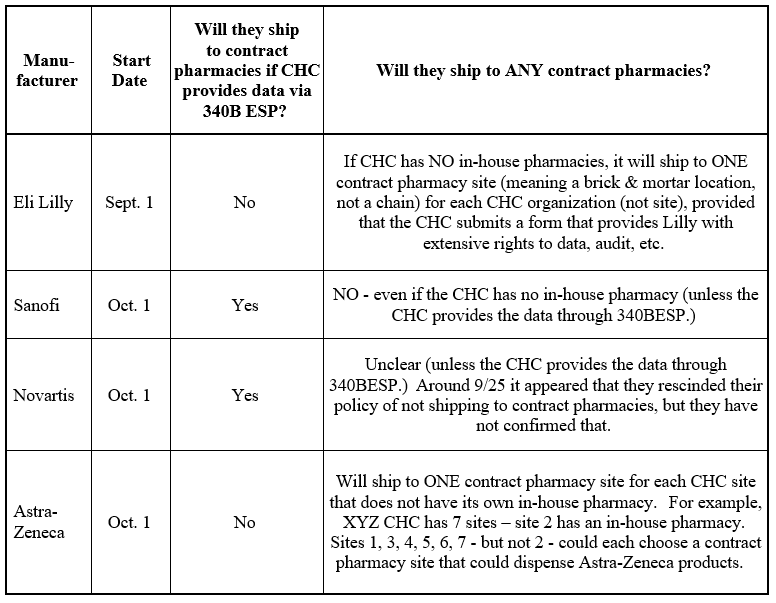
Drug manufacturers
Four drug manufacturers are potentially scheduled to stop shipping 340B priced drugs to most contract pharmacies starting today, October 1, 2020. Eli Lilly, Astra Zeneca, and Sanofi have all
indicated their intent to stop shipping to contract pharmacies as they’ve done in the past and Novartis has given indication that they will NOT discontinue 340B pricing as of October 1, but this has not been confirmed. The four manufacturers each have slightly different rules around their new restrictions. The chart below summarizes those changes.
|
|
|
|
|
|
|
NACHC Lawsuit Update
The National Association of Community Health Centers (NACHC) is moving forward with a lawsuit and is on schedule to have a complaint filed next week through their attorneys at Feldesman Tucker. NACHC intends to file suit alone instead of including primary
care associations (PCAs) or health centers as plaintiffs for the sake of expediency. However, they are still asking for health centers’ help with the lawsuit. Specifically, they need health centers to prepare "declarations" to be submitted as part of the case, after the initial complaint is filed. A declaration is a short, written statement describing the clinical or operational harm resulting from the manufacturers’ actions, to demonstrate and support the legal allegations of injury.
NACHC and Feldesman Tucker will hold a joint webinar at 2:00 pm CT this Friday, October 2, to provide information about how to prepare and submit a declaration. Their goal is to have multiple declarations from around the country in draft form by the end of next week. Below is the link to join the webinar. The information
on declarations will take place in the first part of the webinar. The second half of the webinar will be a discussion with PCAs on reaching out to their State Attorney General on taking legal action in response to the manufacturers’ actions. Health centers are welcome to stay on for that portion of the call, but the first part of the call will contain the most pertinent information.
1-866-469-3239. Code 632 274 023 #
|
|
|
|
|
Executive Order on Access to Life-saving Medications Proposed Rule Summary
The new regulation implementing the president’s executive order (EO) 13937 around insulin and EpiPens will include a notice of proposed rulemaking (NPRM). The U.S. Health and Human Services Department (HHS) has issued a NPRM that includes a comment period ending on October 28.
The proposed requirement for all awards under section 330(e) is as follows:
- If a health center is enrolled in the 340B Drug Pricing Program it must have established practices to make insulin and injectable epinephrine available to low-income health center patients who either have insurance with a high cost sharing requirement for either insulin or injectable epinephrine, a high unmet deductible, or who have no health insurance—at or below the price the health center paid through the 340B Drug Pricing Program, plus a minimal administration fee.
- This requirement applies to low income health center patients only. An individual would not be considered a "patient"
of the health center for this purpose if the only service received by the individual from the health center is the dispensing of a drug or drugs.
- Low-income health center patients are defined as those individuals or families with annual incomes at or below 350% of the Federal Poverty Guidelines.
- This requirement is limited to increasing affordable access to insulin and injectable epinephrine and does not apply to other 340B drugs.
- Nothing in this Program Term or the actions described in this NPRM prohibits or otherwise restricts a health center from setting the price for insulin or injectable epinephrine lower than the price the health center paid through the 340B Drug Pricing Program.
- The "minimal administration fee" would be expected to include any dispensing fee, counseling costs, and any other charges associated with the patient receiving the medication. As the fee must be "minimal," the administration fee should not create a
barrier to low income patients accessing these drugs, and health centers should make every reasonable effort to keep the fee as low as possible. Health centers may consider referring to the Medicaid dispensing fee in their state as a comparison for what may be considered a minimal administration fee. Please note that when there is a separate fee associated with provision of the pharmaceutical service, such as a dispensing fee, health centers must apply a sliding fee discount to that fee.
|
|
|
|
|
South Dakota Legislative Update
|
|
|
|
|
The South Dakota State Legislature held field hearings over the last two weeks to gather input on how the state should spend its $1.25B in Coronavirus Aid, Relief, and Economic Security (CARES) Act relief dollars. There are $597 million in unexpended dollars available that need to be spent by December 31.
Jill Franken, CHAD board member, Falls Community Health executive director, and Sioux Falls Health Department public health director, provided testimony to the Joint Health and Human Services (HHS) committee with recommendations for spending on September 22, 2020. The recommendations included investing in a robust testing program and planning for the distribution of an eventual vaccine. CHAD requested that any program opened up to businesses for grant relief also be made available to nonprofit organizations.
The committee listened to several hours of testimony and provided a list of recommendations to the Joint Appropriations Committee. The Joint Appropriations Committee met on September 29. Their objective was to review the recommendations of the various policy committees for the COVID-19 CARES funds available to the state. The Committee passed a recommended resolution to be considered by the full Legislature at a Special Session on October 5. The recommended resolution does not have the force of law but provides the framework by which the committee is recommending the money is allocated. The recommended resolution includes:
$400 million for Small Business COVID Interruption grants. The grants are a maximum of $100,000 and any federal funding received must be deducted from small business losses in determining the grant amount. The grant applications are proposed October 12 and must be spent by December 30.
$40 million for non-profit business interruption grants. The maximum is $100,000 and any federal funding received must be deducted. The program otherwise mirrors the for-profit program.
$10 million for start-up business COVID Interruption grants. The maximum is $100,000 and can be used for renovation, inventory or equipment purchases made for a business that was operational on June 1
with losses due to no revenue.
$115 million for Community Based Health Care Providers and health care providers through September.
Providers funded through Medicaid Program, including assisted living, nursing homes, community support providers, residential youth senior homecare, adult services, assistive daily living services providers and ICF providers are eligible to receive these funds.
Grants based on reduction in business comparing the time periods of March through September of 2019 and March through September of 2020. Reduction in business will be calculated by subtracting the 2020 revenue from the 2019 revenue and adding in any federal aid that was previously received as a result of the pandemic.
This fund will be based on a prorated share of available funds.
This fund is not specifically allowing for isolation upgrade grants or any testing support. A facility would have to use grant dollars to address isolation or add testing capacity.
$15 million for acute care in hospitals through September. This money would allow hospitals to cover costs through September. There is an anticipation there will be additional federal assistance after the election and this number will be increased at that time.
$2 million for workforce development and non-accredited institutions for programming to assist with job training in areas like meat packing to assist with COVID 19 business demand increases.
$5 million to Destination Marketing Organizations to promote South Dakota in an effort to capture lost tourism spending during the early COVID-19 shutdowns.
$10 million in housing assistance to be used for rent and utility assistance programs for tenants impacted by COVID-19.
These recommendations will now be presented to the full legislature for their consideration. The draft resolution can be found here.
|
|
|
|
|
CHAD 2019 UDS Data Books Presentation – October 21
|
|
|
|
|
Join the Community HealthCare Association of the Dakotas (CHAD) on Wednesday, October 21, at 1:00 pm MT/ 2:00 pm CT for a comprehensive overview of the 2019 CHAD and Great Plains Health Data Network (GPHDN) Data Books. The CHAD team has prepared the books for their member health centers and the GPHDN using the most current data from the Uniform Data System (UDS). These publications were created for use within the CHAD and GPHDN networks and are not publicly shared.
This presentation will walk members through the contents and layout of the 2019 CHAD and GPHDN Data Books. Presenters will provide an overview of the data and graphs that demonstrate trends and comparisons in patient demographics, payor mixes, clinical measures, financial measures, and provider productivity. The session will wrap-up with a glance at individual health center data snapshots. This meeting will provide an excellent opportunity for members to ask questions and share the background story behind the data. Registration information with links to the 2019 CHAD and GPHDN Data Books is coming soon.
|
|
|
|
|
Save the Dates for the 2020 UDS Training Sessions
|
|
|
|
|
| Save the dates for the 2020 Uniform Data System (UDS) training sessions on November 5, 12, and 19 in the afternoon. These FREE web-based trainings are designed to provide assistance navigating and preparing the 2020 UDS report. This training is for people of all levels of prior UDS experience and covers all aspects of the UDS report. The first two sessions will allow participants to gain an understanding of the UDS tables and forms, learn about new measures and requirements, and learn tips for success
in completing your report. The final session will be an hour-long Q&A meeting.
Effective reporting of a complete and accurate UDS submission depends on understanding the relationship between data elements and tables. This interactive training is an excellent way for new staff to understand their UDS reporting effort role. This training has been designed for attendees of all levels. All financial, clinical, and administrative staff are invited to learn updates, hone reporting skills, and share questions and experiences with their peers. Registration link coming soon.
|
|
|
|
|
CMS Shares Medicaid and CHIP Data Showing a Decline in Children’s Care
|
|
|
The Centers for Medicare and Medicaid Services (CMS) recently announced an analysis of Medicaid and the Children’s Health Insurance Program (CHIP) data that shows a sharp decline in children’s care, including childhood screenings, mental health, and dental care. Compared to this time last
year, the analysis noted a 22% drop in vaccinations, a 44% drop in screenings, a 44% drop in mental health services, and a 69% drop in dental visits. In its urgent call to action, CMS highlighted the flexibilities they have provided states, including telehealth and allowing pharmacists to administer vaccinations, and called on partners, including health centers, to work together to address this critical public health issue.
|
|
|
|
|
FCC Funding Deadline Extended
|
|
|
|
|
The Federal Communications Commission’s (FCC) Wireline Competition Bureau (WCB) awarded members of the Great Plains Health Data Network (GPHDN) $443,417.00 for the COVID-19 Telehealth Program in June 2020. The original deadline to purchase and implement eligible services and devices was September 30. On September 28, the WCB extended the deadline to December 31. The GPHDN will use the extra time to confirm FCC approval on all submitted expenses and ensure we are maximizing use of the available funds. The WCB received several extension requests and, considering the continuing impact of the COVID-19 pandemic, they believe that extending the purchase and implementation deadline is reasonable under the circumstances and is also consistent with the purpose of the Coronavirus Aid, Relief, and Economic Security (CARES) Act. The full public notice can be found here. The COVID-19 Telehealth Program has provided $200 million in funding, appropriated by the CARES Act, to help health care providers provide connected care services to patients at their homes or mobile locations in response to COVID-19. The program provides immediate support to eligible providers responding to the pandemic by funding their telecommunications services, information services, and devices necessary to provide critical connected care services. The FCC issued funding awards until the $200 million budget was exhausted, which was a total of 539 applications.
|
|
|
|
|
CHAMPS/ NWRPCA Virtual Primary Care Conference October 19-22
Submitted by CHAMPS
|
|
|
|
|
|
|
The Community Health Association of Mountain/Plains States (CHAMPS) and the Northwest Regional Primary Care Association (NWRPCA) virtual primary care conference, Leading in a New Landscape, will take place October 19-22, and registration is now open! This year’s theme reflects the extraordinary
times we are all facing and the exceptional and inspiring leadership of Region VIII community health centers. Participants will have the opportunity to attend an opening plenary featuring Health Resources and Services Administration’s (HRSA) Jim Macrae and Dr. Luis Padilla, special sessions about the upcoming election and 340B, 30 educational sessions, roundtable peer-networking sessions, and more. For more information and to register, click here. To view the draft agenda and session information, click here. To register for the FREE opening plenary, click here.
|
|
|
|
|
National Substance Abuse Prevention Month: Ask and Educate
|
|
|
|
|
|
|
October is National Substance Abuse Prevention Month, and this year it seems especially important to focus efforts on substance abuse prevention. While this has always been an important topic, COVID-19 has made it even more urgent. Research has indicated that there is a link between substance abuse and COVID-19 susceptibility, both because of the effect the virus can have on people with compromised health and because of the social situations that put them at greater risk of contraction. Community health centers in North Dakota and South Dakota play a vital role in preventing substance use disorders. Some health centers have implemented Screening, Brief Intervention and Referral to Treatment (SBIRT), while others are providing screening and treatment services such as medication assisted treatment (MAT) or addiction and mental health counseling. Case management services that utilize
social workers or other professionals to help patients navigate housing, social services, and other stressful areas in a patient’s life are also methods of prevention. To highlight the importance of recognizing National Substance Abuse Prevention Month, CHAD conducted interviews with substance abuse treatment providers in North Dakota and South Dakota to gain their perspective and insights. Please look for interviews with Jamila Brown, family nurse practitioner and MAT provider at Community Health Service, Inc. in Grafton, ND, and Jessica Albrecht, licensed professional counselor and licensed addiction counselor at Horizon Health Care in Alcester, SD, on CHAD’s social
media sites this month. The Departments of Health in both North Dakota and South Dakota have resources to support providers and patients dealing with substance use concerns. North Dakota has an entire website dedicated to providing the public and
providers with information on how they can participate in preventing substance abuse. South Dakota also has a website dedicated to prevention services, focusing specifically on opioid and methamphetamine addiction. South Dakota also offers
a free online training to health care providers on implementing SBIRT in a medical setting.
|
|
|
|
|
SUD and Breast Cancer Social Media Materials Available
|
|
|
|
|
|
|
October is a busy month for health centers. National Breast Cancer Awareness Month and the National Substance Use Prevention Month both provide an opportunity to raise awareness about the importance of education, screening, and prevention. Use the toolkits’ images and copy to spread the word and promote events and screening
opportunities. These resources are customizable by health centers. A link to materials has been sent to members of the CHAD marketing network team. Contact Kayla Hanson for access. Check out CHAD’s
Facebook page and Twitter account to see (and share!) these important public health
messages.
|
|
|
|
|
|
|
|
|
|
|
South Dakota Department of Health COVID-19 Update The South Dakota Department of Health hosts a weekly COVID-19 webinar for health care facilities, medical
providers, laboratorians, long-term care facilities, EMS providers, and other health professionals.
Thursdays in October (reoccurring)
10:00 am MT/ 11:00 am CT
For weekly call-in information, please join the listserv here. Find archived calls and slides here.
|
|
|
|
|
CCHN/CHAMPS Health Equity Learning SeriesSubmitted by CHAMPS The four-part 2020 Health Equity Learning Series hosted by the Colorado Community Health Network (CCHN)/Community Health Association of Mountain/Plains States (CHAMPS) is designed to introduce all levels of staff to the community health center movement’s position and continued efforts in the journey towards a more equitable and just health system. Participants will come away from the series with a greater understanding of organizational and personal positions in this work and a few strategies to assist in moving the work forward. This series is free for all Region VIII health centers, and recordings of each session will be available for at least one year. To access the first three session recordings, click here. Tuesday, October 13
12:00-1:15 pm MT/ 1:00-2:15 pm CT
For more information and to register, click here
|
|
|
|
|
National Diabetes Prevention Program: Lessons Learned for PCAs and Health Centers In fall 2019, the Association of Asian Pacific Community Health Organizations (AAPCHO) and National Nurse-Led Care Consortium (NNCC) co-facilitated a national webinar and four-part learning collaborative for health center
and Primary Care Association (PCA) stakeholders. These HRSA-sponsored training and technical assistance opportunities provided an overview of the CDC’s evidence-based National Diabetes Prevention Program (National DPP) program to improve access to care and prevent type-2 diabetes through health promotion and lifestyle change programs. The purpose is to increase health center awareness of the National DPP program in order to increase access to preventative care for at-risk health center patients.
AAPCHO and NNCC are hosting a progress-to-date webinar with federal updates from the Health Resources and Service Administration (HRSA) and the Centers for Disease Control and Prevention (CDC) leaders as well as highlight lessons learned and diabetes prevention best practices for health centers and primary care associations (PCAs). This webinar is intended for community health centers, PCAs, health center controlled networks (HCCNs), and organizations interested
and/or invested in National DPP programming within the health center program. Wednesday, October 14
11:00 am MT/ 12:00 pm CT
Register here.
|
|
|
|
|
Telehealth Considerations and Strategies for Special and Vulnerable Populations
This webinar will focus on strategies to reach and serve special and vulnerable populations using telehealth. Special and vulnerable populations include migratory, seasonal, and agricultural workers (MSAW), older adults, people experiencing homelessness, people with limited English proficiency, and rural communities with limited access to broadband. Speakers will discuss building the awareness,
knowledge, and ability of both patients and health center staff to successfully use telehealth to meet the needs of these important groups. They will also share how telehealth promotes health equity and increases overall access to quality health care for special and vulnerable populations.
This webinar is being presented through a partnership of four Health Resources and Service Administration (HRSA)-funded national training and technical assistance partners: NCECE, NCFH, CSH, and HITEQ. Thursday, October 15
12:00 pm MT/ 1:00 pm CT
Register here.
|
|
|
|
|
Integrating HIV Care, Treatment, & Prevention Services into Primary Care
Presented by the Dakota
AIDS Education & Training Center (DAETC), this webinar will provide promising practices for integrating HIV services into primary care, including promoting sexual health and routine HIV screening as a standard of care and provide practical strategies for implementing pre-exposure prophylaxis (PrEP) in a primary care setting. The presenter will describe how to create a "one-stop-shop" for individuals to receive integrated services and identify how to enhance EHR systems to improve HIV services integration.
Thursday, October 15
11:00 am MT/ 12:00 pm
CT
Register here.
|
|
|
|
|
Clinician Technical Assistance Office Hours: The Management of Alcohol Use Disorder Please join the National Clinician Consultation Center in partnership with the Health Resources and Services Administration’s Bureau of Primary Health Care for this interactive webinar for health center clinicians. Unhealthy alcohol use remains a growing public health issue in the United States, contributing significantly to the global burden of disease and posing challenges to the everyday practice of primary care. In this webinar, presenters will define the spectrum of unhealthy alcohol use and compare therapeutic approaches, focusing on pharmacological treatment options. They will also provide strategies for managing withdrawal, an especially important issue during COVID-19. Following this webinar, participants will be
able to assess and care for patients with unhealthy alcohol use more confidently. Thursday, October 22
11:00 am MT/ 12:00 pm CT
Register here.
|
|
|
|
|
| CHAD Network Team Meetings
Tuesday, October 13 at 1:00 pm MT/ 2:00 pm CT – Communications and Marketing Network Team
Friday, October 16 at 11:00 am MT/ 12:00 pm CT – Behavioral Health Work Group
Tuesday, October 27 at 12:00 pm MT/ 1:00 pm CT – O & E Network Team
|
|
|
|
|
|
|
|
|