|
|
|
|
|
|
As the number of COVID-19 cases in North Dakota and South Dakota continues to climb, it is important to understand the number of positive cases alongside both the positivity rate and the number of hospitalizations. For both states, the climbing rates of hospitalizations and the climbing positivity rate confirm what we know at the provider level: we have a serious problem with COVID-19 spread. In particular, the positivity rate tends to vary depending on who is reporting the data; we thought a deeper dive into the numbers could be helpful.
Let’s start
with North Dakota because they have been transparent about their methodology, and they have worked to align it with national reporting. Check out this helpful Facebook post by Ben Schram, an epidemiologist in the North Dakota Department of Health Division of Disease
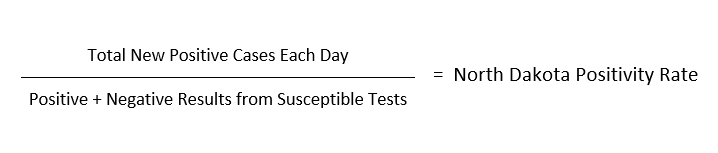
Control. North Dakota calculates their positivity rate as:
|
|
|
|
|
They define susceptible tests as the total number of individuals who were tested that day (so if their test was run twice in that day, perhaps using different methods, they are only counted once) who have NOT previously tested positive. Based on the numbers posted on the North Dakota Department of Health dashboard on November 4 there were 8,377 total tests, 7,886 susceptible tests, and 1,116 positive cases. Using the total positive cases divided by susceptible tests, their daily positivity rate was 14.15%. Their 14-day rolling average was 12.8%. This is comparable to the 7-day rolling average posted by John’s Hopkins of 13.5%.
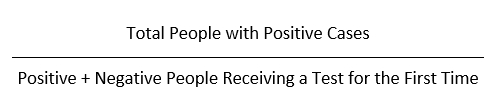
In communication with the South Dakota Department of Health, they have shared that they calculate their positivity rate using:
|
|
|
|
|
More on testing types later, but using their approach, South Dakota had 945 total positive cases posted on November 4 that led to a daily positivity rate of 17.7% and a 7-day rolling average of 19.6%. The 7-day rolling average according to Johns Hopkins was
50.6%.
So, why the big difference between the state and national rates? And, which positivity rate methodology is correct?
The federal government has not issued guidance on the "right" approach to calculating positivity, making it difficult to compare rates across states and between data sources. If you’re interested in learning more, check out this blog post by the COVID Tracking Project.
Having said that, we know there are three typical ways a positivity rate can be calculated. The South Dakota DOH way (also used by the Center for Disease Control), the North Dakota DOH way (which seems to have the blessing of the COVID-19 Tracking Project), and a third approach, which we suspect is being used in the Johns Hopkins calculation of South Dakota’s
rate using:
|
|
|
|
|
Using the numbers from North Dakota’s dashboard (South Dakota doesn’t have similar numbers available on their site), we can illustrate the possible variation in positivity rates using the three methodologies:
|
|
|
|
|
Johns Hopkins states that they vary in the methodology used based on the numbers that each state reports. This does call into question the comparability of their data from state to state, and it is hard to see how it is an accurate assessment of the total testing taking place in a state.
Regardless of the methodology used, the North Dakota and South Dakota positivity rates are too high. The World Health Organization suggests that a positivity rate over 5% indicates that the state is only testing the sickest patients who seek medical care and is failing to cast a wide enough net to identify milder cases and catch outbreaks early. Neither state comes close to 5% under any methodology.
When the positivity rate is used in combination with the rising number of cases in the two states, we can surmise that 1) we have dangerous growth in the number of COVID-19 cases, and 2) it is NOT solely explained by the fact that we are doing more testing. This is confirmed by hospitalization rates, which are not impacted at all by the number of tests being offered. North Dakota and South Dakota are two of the highest states in the nation in their per population rate of hospitalization.
On the ground, we do observe that Governor Burgum has put an enormous amount of effort into supporting testing, including testing events that increase access to COVID-19 tests. That is borne out in the numbers in a couple of ways. First, North Dakota has done nearly double the cumulative number of tests over the course of the pandemic: 901,043 compared to 450,431 in South Dakota. In addition, even as cases rise, North Dakota has a lower positivity rate
with a 12.8% 14-day rolling average compared to a 19.6% 7-day rolling average in South Dakota.
Finally, a word about antigen testing. (For a quick primer on testing types, check out this CHAD article.) Antigen testing (affordable, rapid tests that can be done in clinics, nursing homes, and schools) is quickly becoming an important part of our national testing strategy. The federal government purchased 150 million antigen tests and distribution began to states in September. Clearly, it will be important for all states to accurately report antigen testing rates and results, but so far there is not consistency in how states are reporting antigen tests. Right now, North Dakota does not report antigen tests either in their count of positive cases or in their positivity rate. South Dakota has begun to report antigen test positives as "probable cases" in its total number of COVID-19 cases, but they are not included in its positivity rate. This is consistent with current CDC guidelines, but one would hope that CDC and their federal partners would continue to evolve their reporting approach as antigen testing becomes more widespread and more central to our national testing strategy.
In conclusion, as you consider positivity rates, the rates being shared by the North Dakota and South Dakota Departments of Health are probably the most reliable metrics we
currently have. When our positivity rates of 12.8% and 19.6% are considered in conjunction with our high per population rates of positive cases and hospitalizations, we can confirm that we have serious outbreaks underway in both states. As both states’ testing systems are being strained by current demand, attention to continued access to timely test results is critical, and increased access to antigen testing will be part of the solution.
|
|
|
|
|
|
|
|
|
Horizon Health Care celebrated the opening of its new Yankton location with a ribbon cutting in October.
|
|
|
|
|
|
|
Northland Health Centers Rolla staff decorated this cute haybale for a local contest.
|
|
|
|
|
|
|
|
|
|
|
Horizon Health Care’s Dr. Tom Dean was interviewed about the virus surge by multiple outlets, including the Associated Press, NBC News, and KELO.
|
|
|
|
|
|
|
|
|
Spectra Health is working on expanding its downtown Grand Forks facility via the Grand Forks Herald.
|
|
|
|
|
|
|
|
|
|
|
|
|
| Top Counties and Trends in the Dakotas
|
|
|
|
|
|
|
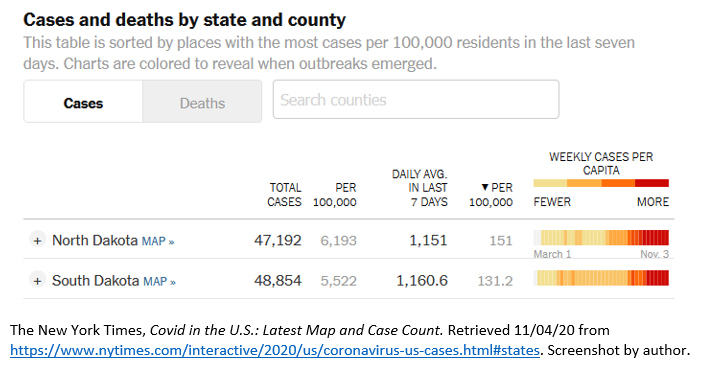
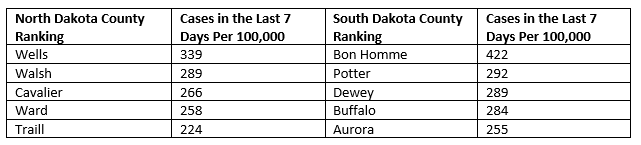
As of Wednesday, November 4, North Dakota and South Dakota remain ranked 1 and 2 in total new cases per population over the last seven days, according to the New York Times COVID-19 database.
The emerging hot spots in the two states with the most cases in the last seven days per population are:
|
|
|
|
|
|
|
|
|
|
|
Updates to State Contact Tracing Approaches
|
|
|
|
|
North Dakota
On October 20, North Dakota Governor Doug Burgum announced changes to the state’s contact tracing process. Due to the spike in cases in recent weeks and the large backlog in positive cases to be notified, North Dakota suspended close contact tracing and notification by public health officials. Positive individuals will still be notified by public
health but are being instructed to self-notify their close contacts and direct them to the North Dakota Department of Health (NDDOH) website. According to Governor Burgum, the backlog has been successfully completed, and it is unclear if this new contact tracing process will be permanent.
Below is guidance for providers and the public on talking points for close contacts.
- The NDDOH has
discontinued close contact notification and investigation. As a result, information about household and close contacts are not collected or known by the NDDOH.
- COVID-19 cases are asked to notify their household and close contacts about their exposure. This information is not reported back to the NDDOH.
- The NDDOH is no longer able to provide quarantine letters for household and close contacts.
- Isolation letters will be provided to COVID-19 cases if requested.
- Schools, childcare centers, businesses, and organizations should not require documentation from the NDDOH that an individual is quarantined due to COIVD-19 exposure. They should also not require NDDOH documentation so a contact can go back to school, sports, or work.
- Individuals can reach out to the Department of Labor at 701-328-2660 with their concerns about an employer insisting NDDOH quarantine documentation is needed.
- Official documentation from the NDDOH is not needed the Families First Coronavirus Response Act (FFCRA) funding reimbursement.
South Dakota
Secretary of Health Kim Malsam-Rysdon updated the media on the South Dakota Department of Health (SDDOH) contact tracing during the October 21 press briefing. Over 300 people are working on contact tracing seven days a week for approximately 12 hours a day. The SDDOH is onboarding another group of National Guardsmen to assist with contact tracing. With the limited time and resources, the SDDOH prioritizes students and teachers, people in congregate settings, and people over 65.
|
|
|
|
|
Provider Relief Fund Deadline for Applications November 6
|
|
|
|
|
On October 22, the Department of Health and Human Services (HHS) announced that it is amending the reporting instructions to increase flexibility around how providers can apply provider relief fund (PRF) money toward lost revenues attributable to coronavirus. After reimbursing health care-related expenses attributable to coronavirus unreimbursed by other sources, providers may use remaining PRF funds to cover any lost revenue measured as a negative change in actual year-over-year revenue from patient care-related sources. In essence, this change removes the September 19 reporting requirement and rolls the instructions back to the guidance issued in June. Applications are still being accepted for Phase 3 of the PRF. Applications may be submitted here until November 6.
|
|
|
|
|
|
|
|
|
CHAD continues to monitor developments around 340B. Listed below are the latest updates:
- South Dakota Congressman Dusty Johnson is a co-author of a "Dear Colleague" letter currently circulating in the US House of Representatives. CHAD has put in a request to North Dakota Congressman Kelly Armstrong’s office to sign onto the letter. The
Spanberger-McKinley letter asks that the Department of Health and Human Services (HHS) not to make 340B a rebate program. The deadline to sign the letter has been extended to Friday, November 6.
- The National Association of Community Health Centers (NACHC) led a Twitter chat this week that was very successful. The #Protect340B hashtag appeared on 25,000 timelines during the hourlong chat. In the coming days, there will be a follow-up, including key statistics and key quotes posted during the chat. There are resources available from NACHC for 340B advocacy, and the toolkit can be found here.
- CHAD will be coordinating some earned media and social media efforts in the coming weeks. We plan to reach out for some collaborations on that effort; more information to come in the next couple of weeks.
- CHAD submitted comments to HRSA regarding the notice of proposed rulemaking around the implementation of the Executive Order on EpiPens and insulin by the October 28 deadline.
- CHAD still has technical assistance hours available with Matt Atkins from Draffin Tucker. If you could use those hours, please feel free to reach out to
Jessica Gilbertson.
- Please visit our 340B resource page for updates and more information.
|
|
|
|
|
2020 UDS Training Sessions Begin Today
|
|
|
|
|
Join CHAD for the 2020 Uniform Data System (UDS) training sessions on November 5, 12, and 19 from 1:30 pm-4:30 pm CT. These FREE web-based trainings are designed to provide assistance navigating and preparing the 2020 UDS report. This training is for people of all levels of prior UDS experience and covers all aspects of the UDS report. The first two sessions will allow participants to gain an understanding of the UDS tables and forms, learn about new measures and requirements, and learn tips for success in completing your report. The final session
will be an hour-long Q&A meeting.
Effective reporting of a complete and accurate UDS submission depends on understanding the relationship between data elements and tables. This interactive training is an excellent way for new staff to understand their UDS reporting effort role. This training has been designed for attendees of all levels. All financial, clinical, and administrative staff are invited to learn updates, hone reporting skills, and share questions and experiences with their peers. Register here.
|
|
|
|
|
Health Centers Participate in Youth SBIRT Learning Collaborative
|
|
|
|
|
In July, CHAD participated in a focus group for the National Council for Behavioral Health to discuss the potential benefits of primary care associations and health centers working with the National Council to implement youth screening brief intervention and referral to treatment (SBIRT) in primary care. In September, Horizon Health Care, Spectra Health, and the Community Health Center of the Black Hills joined CHAD in applying to be part of the National Council’s youth SBIRT learning collaborative. CHAD recently learned that the group is one of three PCA/health center partnerships to be selected for the collaborative learning cohort starting in January 2021.
The collaborative is six months long and will familiarize health centers with the screening to brief intervention (S2BI) screening tool, provide education regarding youth substance and alcohol abuse, assist in creating a work plan, provide resources and tools for data collection, and ultimately lead to the implementation of youth SBIRT in these health centers. CHAD is thrilled to be involved and grateful to the health centers for their willingness to participate and enhance these necessary services for the youth they serve.
|
|
|
|
|
USPSTF Draft Recommendation for Colorectal Cancer Screening Lowering Age to 45
|
|
|
|
|
The United States Preventive Services Task Force (USPSTF), an independent, volunteer panel of national experts in prevention and evidence-based medicine, has released a draft recommendation statement on screening for colorectal cancer. Click here to review the draft statement. Public comments on the draft statement can be submitted through November 23.
The American Cancer Society (ACS) has provided key points regarding the draft recommendation statement:
- The updated draft recommendations are in line with ACS’s recommendations regarding colorectal cancer screenings for average-risk populations;
- The new guidelines lowered the age to start screening from 50 to 45 and recommend continuing regular screening until age 75;
- The guidelines still classify
screening from age 50-75 as grade "A" but have added 45-50 as grade "B";
- Under the Affordable Care Act (ACA), compliant plans must cover screenings with both A and B ratings;
- The guidelines recommend the decision to screen those aged 76 to 85 years be individualized based on screening history and overall health status and classify that age group a grade "C"; and,
- USPSTF’s guidelines are for average-risk populations only. USPSTF does not draft guidelines for high-risk populations.
|
|
|
|
|
Introducing the GP11 Network News
|
|
|
|
|
|
|
The Great Plains Health Data Network (GPHDN) would like to introduce the GP11 Network News in this edition of the newsletter! Each CHAD newsletter will contain a GP11 Network News section highlighting different health information technology initiatives happening in the network. Topics may include educational opportunities, program updates, or upcoming events. Please contact Becky Wahl or Kyle Mertens to include any noteworthy news that should be shared with other health centers.
|
|
|
|
|
Great Plains Health Data Network Website is Live
|
|
|
|
|
The Great Plains Health Data Network (GPHDN) website has launched. The website, GPHDN.org, can also be found by going to the Community Healthcare Association of the Dakotas (CHAD) website and looking under Partners & Affiliates. The website provides the network’s mission and shows the 11 participating health centers in the Health Center Controlled Network (HCCN) that began in August 2019. Learn more about the GPHDN leadership committee and partners working together to advance the participating health centers’ mission across the Dakotas and Wyoming. Current webinars and events, along with the registration links, are included on the website. Check out the media center for the latest news and information about GPHDN and the participating health centers to include the recent newsletters for CHAD and the Wyoming Primary Care Association (WYPCA) and press releases. Finally, this website will allow the GPHDN to share valuable resources with participating health center staff to include webinar
recordings, PowerPoint presentations, and workgroup documents. These resources are only available to GPHDN members; a login will be required to access this information. If you need assistance with your website login information, please contact Kayla Hanson.
|
|
|
|
|
Open Enrollment Underway in the Dakotas
|
|
|
|
|
|
|
The 2021 open enrollment period has begun! Insurance plans and pricing can change every year, and patients are encouraged to compare plans and actively re-enroll. Many people may benefit from a change, and the marketing toolkit CHAD will distribute this month directs people to visit www.healthcare.gov for more information and call and make an appointment if needed.
|
|
|
|
|
November is National Diabetes Awareness Month
|
|
|
|
|
November is National Diabetes Month, and communities across the country are teaming up to bring attention to diabetes. Almost 1 out of every 16 health center patients in the Dakotas have a diagnosis of diabetes. Community health centers are specially equipped to help patients improve diabetes outcomes by integrating behavioral, oral, and primary health care and addressing barriers to care. Health centers offer whole-person care, which means we can work to help patients overcome the
barriers that might prevent them from becoming and staying healthy.
|
|
|
|
|
|
|
|
|
|
|
|
|
South Dakota Department of Health COVID-19 Update The South Dakota Department of Health hosts a weekly COVID-19 webinar for health care facilities, medical
providers, laboratorians, long-term care facilities, EMS providers, and other health professionals. Thursdays in November (reoccurring)
10:00 am MT/ 11:00 am CT
For weekly call-in information, please join the listserv here. Find archived calls and slides here.
|
|
|
|
|
South Dakota Department of Health COVID-19 Mass Vaccination Planning
The South Dakota Department of Health hosts a weekly COVID-19 vaccination planning webinar for health care facilities, medical providers, laboratorians, long-term care facilities, EMS providers, and other health professionals.
Tuesdays (reoccurring thru March 2021)
12:00 pm MT/ 1:00 pm CT
Meeting link or call (669) 900 9128
Meeting ID: 845 2763 1820
Passcode: 719500
|
|
|
|
|
Understanding the Ground: Social Determinants of Health in Rural Populations
Building on work conducted by the Rural and Minority Health Research Center, this presentation will review some of the key elements associated with health across rural White and minority populations, such as education, income, and health facility availability. The webinar is free, no registration is required, but participation is limited to the first 500 to log-on that day. If the webinar reaches capacity, you will be able to access the recording archived on the Gateway website. Tuesday, November 17
11:00 am MT/ 12:00 pm CT
Link to join.
Dial-in Number: 800-369-3138
Participant Passcode: 7338676
|
|
|
|
|
COVID-19 in North Dakota: Mental Health and Public Health
Presented by the North Dakota Rural Health Association, this webinar will look at the
pandemic’s effect on mental health and public health in North Dakota and the resources available. Click here for more information.
Thursday, November 19
11:00 am MT/ 12:00 pm CT
Link to join. No registration is required.
|
|
|
|
|
Organizations Values, Culture, and Measurement: Impact
on the Bottom Line
Presented by the North Dakota Rural Health Association, this presentation will provide both concepts, models, and case studies to show how rural leaders can answer the call to action to optimize primary care in rural markets. With declining reimbursement and increased competition, independent hospitals, health care systems, and independent practices must leverage available opportunities to improve financial performance. Rural providers and other stakeholders should consider their organizational values and how those are put in action to ensure their advantages can be strategically positioned using an abundance mindset to ensure a measurable impact on primary and specialty care practice alignment within the health care system. Thursday, November 19
12:00 pm MT/ 1:00 pm CT
Link to join. No registration is required.
|
|
|
|
|
Surviving & Thriving – The Power of Rural is 100% Community
On National Rural Health Day, Katherine Ortega Courtney, Ph.D., and Dominic Cappello, authors of 100% Community: Ensuring 10 Vital Services for Surviving and Thriving, will discuss their groundbreaking research and the roadmap they have created to help rural counties press reset and learn how to work together in new ways to create local systems of health, safety, education, and economic stability. Thursday, November 19
12:00 – 1:15 pm MT/ 1:00-2:15 pm CT
Register here.
|
|
|
|
|
| CHAD Network Team Meetings
Tuesday, November 10 at 1:00 pm MT/ 2:00 pm CT – Communications and Marketing Network
Team
Friday, November 20 at 11:00 am MT/ 12:00 pm CT – Behavioral Health Work Group
Tuesday, November 24 at 12:00 pm MT/ 1:00 pm CT – O & E Network Team
Wednesday, November 25 at 10:00 am MT/ 11:00 am CT – Advocacy Network Team
|
|
|
|
|
|
|
|
|